V 1.0 Stroke – Global Challenges, Local Solutions
Abstract
Stroke is the second leading cause of death (after heart disease) and a major cause of disability worldwide. Also called a brain attack, typical symptoms of stroke include sudden one-sided weakness and numbness in the face and arm as well as altered speech. Most strokes are ischaemic strokes where arterial blood flow to the brain is interrupted by an embolism or thrombosis. Strokes are less frequently caused by haemorrhage. Non-contrast cranial computed tomography (CT) imaging, the workhorse of acute stroke diagnosis, can reliably differentiate between ischaemic stroke and intracerebral haemorrhage. Contrast CT imaging – including angiography, perfusion and magnetic resonance imaging (MRI) – can be used to detect large vessel occlusions and to identify ischaemic brain tissue that can still be salvaged by reperfusion. Treatment of acute ischaemic stroke focuses on the rapid reperfusion of brain tissue by means of intravenous thrombolysis and endovascular thrombectomy to salvage the at-risk tissue surrounding the infarct core. Reperfusion therapy is followed by specialised multidisciplinary stroke unit care and rehabilitation, all of which increases the chance of survival and reduces long-term disability. The mainstay of acute haemorrhagic stroke treatment in hypertensive patients is a lowering of blood pressure to stop haematoma expansion. Selected patients benefit from haemostatic agents or surgical treatment. Prevention of recurrent strokes includes lifestyle modifications and therapeutic interventions to control hypertension, hyperlipidaemia, diabetes, and smoking. Specific interventions to prevent recurrent strokes depend on the underlying stroke aetiology. These include antithrombotic medication, anticoagulation for atrial fibrillation, carotid endarterectomy or stenting, and the closure of a patent foramen ovale in ischaemic stroke patients.
Keywords
History
The first description of a stroke by HIPPOCRATES over 2,400 years ago resembles today’s clinical description remarkably well. HIPPOCRATES described a sudden loss of speech, sensation, and power as if the person was “struck down by violence”. However, the biological cause of this dramatic and sudden loss of physical and mental function remained unknown for almost 2000 years. The term “stroke” was coined in the late 17th century by the physician William COLE. Around the same time, the anatomists Jacob WEPFER and Thomas WILLIS recognised that the occurrence of symptoms was related to a disturbed blood supply to the brain. In some stroke patients, they found an occlusion of large blood vessels supplying the brain, in others they observed bleeding into brain tissue. In 19th century Berlin, the pathologist Rudolf VIRCHOW distinguished between ischaemic stroke (Greek: ἴσχειν/is-chein ‘restrain’ + αἷμα/haima ‘blood’), which is caused by the occlusion of a blood vessel, and haemorrhagic stroke caused by blood vessel rupture and bleeding into the brain tissue (Greek: αἷμα/haima ‘blood’ + ῥῆξις/rhēxis ‘burst’).
Definition
Today, stroke is defined as an acute episode of focal dysfunction of the brain, retina, or spinal cord of a vascular origin if symptoms last longer than 24 hours or if computer tomography (CT), magnetic resonance imaging (MRI), or an autopsy show ischaemic brain injury or haemorrhage corresponding to the symptoms. Stroke is differentiated from a transient ischaemic attack (TIA) which is defined as transient neurological dysfunction without evidence of an ischaemic lesion in brain imaging for which symptoms typically last less than one hour and no more than 24 hours.
Epidemiology
Stroke is the second leading cause of death (after heart disease) worldwide. It accounts for more than 6.2 million deaths annually (World Health Organization 2020) with ~70 % of these deaths occurring in low- and middle- income countries (FEIGIN et al. 2015, JOHNSON et al. 2019). In high-income countries, nearly nine out of ten strokes are ischaemic strokes. Strokes are less frequently caused by haemorrhage (about 15 %). In Germany, the percentage of strokes caused by ischaemia, intracerebral haemorrhage, or subarachnoid haemorrhage (a bleeding into the subarachnoid space) is 84, 12, and 4 % respectively (EYDING et al. 2019). Globally, the incidence of haemorrhagic stroke (intracerebral haemorrhage and subarachnoid haemorrhage combined) is 30 %, indicating a higher incidence of haemorrhagic stroke in low- and middle-income countries (Institute for Health Metrics and Evaluation 2020). The global lifetime risk of stroke for men and women (at 25 years of age or older) is 25 % (The GBD 2016 Lifetime Risk of Stroke Collaborators 2018); the age-specific incidence increases exponentially with age, doubling for each decade after age 55 (ROGER et al. 2012). In people under 44 years of age, approximately 50 % of strokes are caused by ischaemia, 30 % by subarachnoid haemorrhage, and 20 % by intracerebral haem- orrhage, indicating more diverse underlying pathogeneses and risk factors in this patient group (SINGHAL et al. 2013). Since 1990, the global age-standardised stroke incidence rate has slightly decreased, whereas the highest incidences of stroke are in East Asia, especially China, followed by Eastern Europe (JOHNSON et al. 2019). Strik- ingly, during the same period, the rate of deaths due to ischaemic and haemorrhagic stroke decreased by almost 40 % across all world regions except for sub-Saharan Africa (JOHNSON et al. 2019). However, as the world’s population increases and ages, and the low- and middle-income countries go through an epidemiological transition from infectious to non-communicable diseases, the overall burden of stroke in terms of the absolute number of people affected or disabled by stroke remains high and is steadily increasing (JOHNSON et al. 2019). In 2016, stroke-related disability was the second leading cause of disease burden worldwide, as measured in disability- adjusted life years (DALYs – the sum of life years lost as a result of premature death and years lived in disability adjusted for severity (Fig. 1, JOHNSON et al. 2019)). In Germany, the social costs for treatment and loss of produc- tivity resulting from stroke amount to around €18 billion a year, with treatment costs accounting for approximately 2 % of total health expenditures in 2017 (LUENGO-FERNANDEZ et al. 2019).
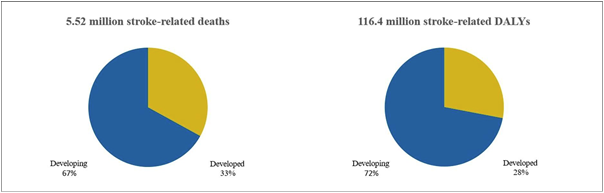
Fig. 1 Stroke-related deaths and DALYs by development status based on the Socio-demographic Index (SDI). Countries with a high and high- middle SDI are summarised under “developed”. Developing countries constitute countries with a low, low-middle, and middle SDI in 2016. The graphs depict absolute numbers as well as a distribution of the bulk of global stroke burden to developing countries (based on JOHNSON et al. 2019).
Tab. 1 Most common symptoms of acute stroke
Sudden onset of:
• Numbness (half-sided)
• Weakness (half-sided)
• Confusion
• Difficulty speaking
• Vision loss
• Dizziness
• Imbalance
• Severe headache
Prognosis
In high-income countries, 10 % to 25 % of stroke patients die within a month, up to a third by the end of year one, and more than half within five years after the initial stroke (LUENGO-FERNANDEZ et al. 2013, SENNFÄLT et al. 2019). Prognosis is even worse for people who experience haemorrhagic strokes, as the 1-month mortality ap- proaches 40 %, indicating the need for improved therapeutic approaches (ASCH et al. 2010). About 50 % to 70 % of stroke survivors regain functional independence. However, 15 % to 30 % suffer from permanent disabilities (particularly hemiparesis, aphasia, sensory loss, spasticity, and an inability to walk unassisted or perform activities of daily living), and about one fifth requires institutional care in a nursing home at 3 months after onset (ROGER et al. 2011). Only about 50 % of working-aged adults return to paid employment within 6 to 12 months after stroke (DANIEL et al. 2009).
Aetiology and Risk Factors
More than 90 % of the overall burden of stroke is attributable to modifiable risk factors, including metabolic risk factors (such as high systolic blood pressure, a high body mass index, high fasting plasma glucose, high total cholesterol, low glomerular filtration rate, and atrial fibrillation) and behavioural risk factors (including smoking, an unhealthy diet, and low physical activity) indicating that preventive programmes aimed at modifying metabolic and behavioural risk factors could lead to a major reduction in global stroke burden (FEIGIN et al. 2016b). Recently, it has become clear that psychosocial factors, including psychosocial stress and depression, also significantly contribute to cerebrovascular risk (HOUSE et al. 2001, SALAYCIK et al. 2007). Strikingly, air pollution has emerged as an additional major modifiable risk factor being attributable to around one-third of the global stroke burden, especially in low- and middle-income countries (FEIGIN et al. 2016b). Hypertensive vascular disease resulting from chronic, increased blood pressure is the most common cause of bleeding into the brain (CORDONNIER et al. 2018); embolisms, mostly from the heart, and large and small vessel thromboses are the most common causes of ischaemic stroke (BOGOUSSLAVSKY et al. 2018).
Pathophysiology
The brain requires a permanent supply of glucose and oxygen to function properly. Although the brain constitutes only 1 % to 2 % of total body mass, it receives 15 % of the resting cardiac blood output and accounts for 20 % of the total body oxygen consumption (FROSCH et al. 2010). The brain is one of the most oxygen-sensitive organs in the body. Here oxygen is used almost entirely for the oxidative metabolism of glucose, which, under normal physiological conditions, is almost the only substrate for the brain’s energy metabolism (CLARKE and SKOLOFF 1999). Oxygen deprivation of the brain may occur through several mechanisms: (i) ischaemia, an either permanent or transient restriction in blood flow, or (ii) hypoxia, a deprivation of adequate oxygen supply caused by low partial pressure of oxygen or a decreased oxygen-carrying capacity of the blood. In addition, haemorrhage results in mechanical damage to brain tissue associated with the mass effect (ARONOWSKI and ZHAO 2011). Following a reduction in blood flow, the survival of the at-risk tissue depends on factors such as duration of the ischaemia, extent of flow reduction, and presence of collateral circulation (FROSCH et al. 2010) or, in the case of a haemor- rhage, haemorrhage volume and intracranial pressure.
The Ischaemic Penumbra
In the late 1970s, ASTRUP et al. (1977) recognised that after the onset of focal brain ischaemia in baboon brains, measurements of neuronal activity revealed regions that were electrically silent but had not yet undergone irre- versible cell death. Blood supply deficiency is severe at the core of an ischaemic stroke, causing irreversible membrane failure and rapid cell death. This infarct core is surrounded by a peripheral zone, the so-called penumbra (Latin: ‘half-shade’) where blood flow deficits are milder and electrical excitability of neurons is lost without causing morphological damage. Strikingly, when cerebral blood is increased, the ability to fire action potentials in these areas is completely restored. But after prolonged ischaemia, widespread cell death ensues. Today, clinical imaging techniques, such as positron emission tomography (PET), allow for real-time visualisation of these areas of ‘stunned’ brain that can be therapeutically salvaged in theory. This discovery has been crucial in changing the way ischaemic stroke has begun being viewed as a potentially “treatable disease” rather than a “preventable catastrophe” (RAMOS-CABRER et al. 2011). Hence, the goal of any circulation restoring strategy is to salvage the at-risk tissue surrounding the infarct core.
Within the ischaemic penumbra, several mechanisms have been identified on a molecular level that irreversi- bly damage brain tissue. In the area with the most severe hypoperfusion, synthesis of adenosine-triphosphate (ATP) drops, while its utilization remains high, leading to acidosis and the dysfunction of energy-dependent ion transporters. As a result, cells swell and membranes rupture. However, ischaemic tissue death is not only caused by the limited availability of ATP, but is a result of a complex interplay between numerous biochemical and cellular events that lead to acute cell death (Fig. 2).
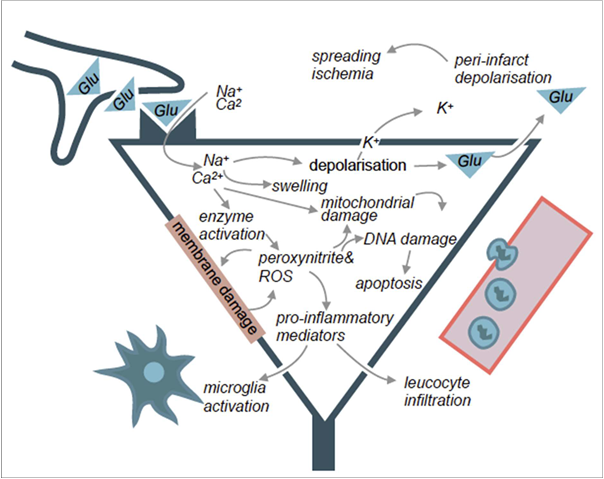
Fig. 2 Biochemical and cellular mechanisms leading to cell death in ischaemic brain tissue.
Excitotoxicity
The metabolic depletion of energy can result in inappropriate release as well as failure of the reuptake mechanisms of excitatory amino acid neurotransmitters, such as glutamate, in depolarizing or dying neurons. Its accumulation in the extracellular space initiates cell damage through prolonged stimulation of α-amino-3-hydroxy-5-methyl-4- isoxazolepropionic acid (AMPA) and N-methyl-D-aspartate (NMDA) receptors, which dramatically increases the influx of calcium, sodium, and water into neurons (ANKARCRONA et al. 1995). This elevation of cellular calcium ions can, in turn, trigger a wide range of harmful processes, including inappropriate activation of catabolic pro- cesses, generation of free radicals, and mitochondrial injury.
Oxidative and Nitrosative Stress
Oxidative and nitrosative stress occur during ischaemia, when the production of free radicals overwhelms the limited scavenging capacity of the brain’s endogenous antioxidants. Free radicals, such as oxygen-derived free radicals and nitric oxide, are molecules with one or more unpaired electrons. They are highly reactive, causing damage and dysfunction to DNA, proteins, and lipids, and potentially lead to cell death (CHAN 2001). Brain tissue damage following the restoration of circulation after a period of ischaemia, a so-called reperfusion injury, is mainly caused by damage from free radicals (SUN et al. 2018).
Cortical Spreading Depolarizations
Electrophysiological studies and imaging data show that cortical spreading depolarization (CSD) occurs sponta- neously in the surrounding tissue of developing infarcts which is metabolically and functionally compromised but has not yet died – i.e. the penumbra (MIES et al. 1993, WOITZIK et al. 2013). CSD, triggered by high levels of extracellular potassium and glutamate that occur during ischaemia, is a highly energy-consuming phenomenon characterised by slowly propagating waves of depolarization of neurons and neuroglia for minutes to days after the onset of stroke (DREIER and REIFFURTH 2015). Expansion of the infarct core is caused by a mismatch of a drastically increased energy demand of activated ion transporters to support membrane repolarization and insuf- ficient delivery of oxygen and glucose to the tissue. This results in neuronal death in energy-deprived tissue (ibid.). Interestingly, stimulation of the brain in critical peri-infarct “hot zones” may cause additional spreading of injury depolarizations via supply-demand mismatch transients and contribute to additional brain injury (BORNSTÄDT et al. 2015).
Mechanisms of Cell Death
Necrosis and apoptosis are the main mechanisms of cell death following ischaemic injury (DIRNAGL et al. 1999). Necrosis and apoptosis can be induced by multiple triggers, including oxidative and nitrosative stress and calcium overload. Mild ischaemic injury preferentially induces delayed neuronal cell death via apoptotic mechanisms, such as activation of caspases, leading to subsequent phagocytosis of the apoptotic bodies (ENDRES et al. 1998). In contrast, necrosis, the passive death of a cell due to severe ischaemia and energy depletion, leads to an uncon- trolled release of inflammatory cellular content and other debris (DIRNAGL et al. 1999). In some cases, neuronal cell death with morphological features of necrosis can be induced by death receptor signalling after ischaemic injury. This receptor-dependent mechanism of cell death has become known as necroptosis (DEGTEREV et al. 2005). Other, more recently identified mechanisms contributing to neuronal death following ischaemic injury include autophagy, a catabolic pathway leading to the self-eating of cellular components by autophagosomes, and phagoptosis, the phagocytosis of eat-me signals which expose stressed but viable neurons (NEHER et al. 2011, WANG et al. 2018).
Inflammation
Inflammation following brain injury is a key contributor to the pathophysiology of stroke. Under conditions of hypoxia, high shear stress, endothelial cell damage, and the generation of reactive oxygen species, the inflamma- tory process begins to unfold in the vascular compartment within minutes after occlusion of an artery. Post- ischaemic inflammation typically follows an orderly process of events involving neurons and neuroglia, vessels, and the circulating blood. Collectively, the ensuing post-ischaemic inflammatory response can be harmful, leading to secondary brain injury. However, post-ischaemic inflammation is a self-limiting process, which, during later stages of the ischaemic injury, is necessary for the removal of dead cells and production of growth factors helping to foster an environment for tissue reconstruction and repair (for review see ANRATHER and IADECOLA 2016). Furthermore, while the immune response starts locally, inflammatory mediators expressed during the early phase of ischaemic damage can propagate through the disrupted blood-brain-barrier (BBB) resulting in a systemic inflammatory response. This, in turn, is followed by an opposing anti-inflammatory response predisposing patients to stroke-induced immunosuppression (for review see: ibid.). Therefore, any therapeutic concept should consider the biphasic nature of post-ischaemic inflammation by attenuating its devastating potential in the acute phase, while enhancing its beneficial contributions to tissue repair during later stages of disease.
Fig. 3 Mechanisms of post-ischaemic damage and protection. The ischaemic cascade is a complex interaction between all cell types of the brain and supplying blood vessels. Permanent injury to brain tissue results from early primary and delayed secondary damage. Necrosis and apoptosis are the main mechanisms of cell death following ischaemic injury. Mild ischaemic injury preferentially induces cell death via apop- totic mechanisms. Apoptosis is the predominant type of cell death in the penumbra. Secondary damage is mostly driven by inflammation through the generation of reactive oxygen species, activation of the complement system, induced apoptosis, and the release of cytotoxic and apoptosis-inducing molecules by cytotoxic T cells and natural killer cells (based on ENDRES et al. 2008).
Difficulties in Translating Stroke Research into Clinical Practice
Despite numerous neuroprotective agents that have been found to reduce brain injury and improve neurological outcomes in various animal models of stroke, the translation of these benefits from the laboratory bench to the stroke unit, the so-called bench-to-bedside translation, has been dismal. In fact, since the early 1960s more than 1,000 molecules with brain-protective effects relevant to stroke have been identified, leading to the publication of more than 3,500 articles and the implementation of several hundred clinical trials aimed at establishing an effec- tive neuroprotective therapy after stroke (O’COLLINS et al. 2006). However, apart from reperfusion induced through mechanical recanalization or intravenous tissue plasminogen activator, translation into effective therapies has failed.
This failure to translate successful preclinical therapeutic candidates into benefits for patients has been described as the translational roadblock or, more dramatically, the translational valley of death, separating the world of preclinical research from clinical benefit. Several reasons for this roadblock and ways to cross the valley of death have been debated in the scientific community but can be regarded along two lines. The first is internal validity. It has been argued that preclinical literature is confounded by factors leading to the overestimation of effect size and identification of false positives. Among the most commonly cited are a prevalence of underpowered studies, lack of measures like randomisation and blinding to reduce bias, and a tendency to avoid the publication of negative findings. According to some meta-analyses, each of these factors can lead to an overestimation of true effect size by 10 – 30 % (CROSSLEY et al. 2008, MACLEOD et al. 2008). At the same time, clinical studies using these false estimates of effect size might be underpowered to detect a true but much smaller effect and thus produce false negatives. The second is external validity in which there is a difference in the stroke models and treatment paradigm in preclinical research and human stroke. One of the most striking differences in many studies compar- ing preclinical and clinical treatment paradigms is the timing of treatment administration. While most preclinical studies administer treatment at the time the ischaemia occurs or even earlier, reaching the patient in real life within
4.5 hours after the onset of symptoms is a challenge. With the advent of new pre-hospital stroke care models, described in more detail below, ultra-early treatment strategies may, however, be within reach in the near future. In addition, inherent differences in the anatomy and physiology of rodent model organisms and humans contribute to the translational roadblock. Even if a pathomechanism proves translatable from mouse to man, differences in the ability of drugs to cross the much weaker barrier between the blood and the brain tissue in model organisms and the human blood brain barrier may lead to a failure of a potential drug to reach the target tissue. Nevertheless, experimental research using animal models of disease has been essential for our understanding of stroke patho- physiology and identifying therapeutic targets (DIRNAGL and ENDRES 2014).
Diagnosis
Typical symptoms of stroke include sudden unilateral weakness and numbness of the face, arm (and leg), as well as altered speech. This has led to the acronym FAST (face, arm, speech, time to call ambulance) to aid prehospital stroke screening and public information campaigns. In essence, all brain functions can be affected by a stroke and indicate a specifically affected brain region – hence the quotation by stroke neurologist C. M. FISHER “we learn neurology stroke by stroke”. Other common symptoms include a sudden onset of non-orthostatic vertigo, visual loss, double vision, unsteady gait, swallowing difficulties, and confusion. Despite sharing a similar clinical presen- tation, acute treatment strategies for haemorrhagic and ischaemic stroke are fundamentally different. Therefore, a fast and reliable distinction between the two stroke types is paramount. Non-contrast cranial computed tomogra- phy (CT) can reliably detect fresh intracranial haemorrhage and remains the workhorse of acute stroke diagnosis. However, its sensitivity for revealing cerebral ischaemia is low for lesions which are recent, small, or in the lower posterior parts of the brain. Acute brain ischaemia can be detected in 90 % of patients with ischaemic stroke by diffusion weighted MRI. Fortunately, MRI also enables clinicians to estimate the onset of stroke in patients with an unclear time of occurrence, for instance when the stroke occurred while the patient was asleep, and thus permits the use of specific acute therapies (Fig. 4, THOMALLA et al. 2018).
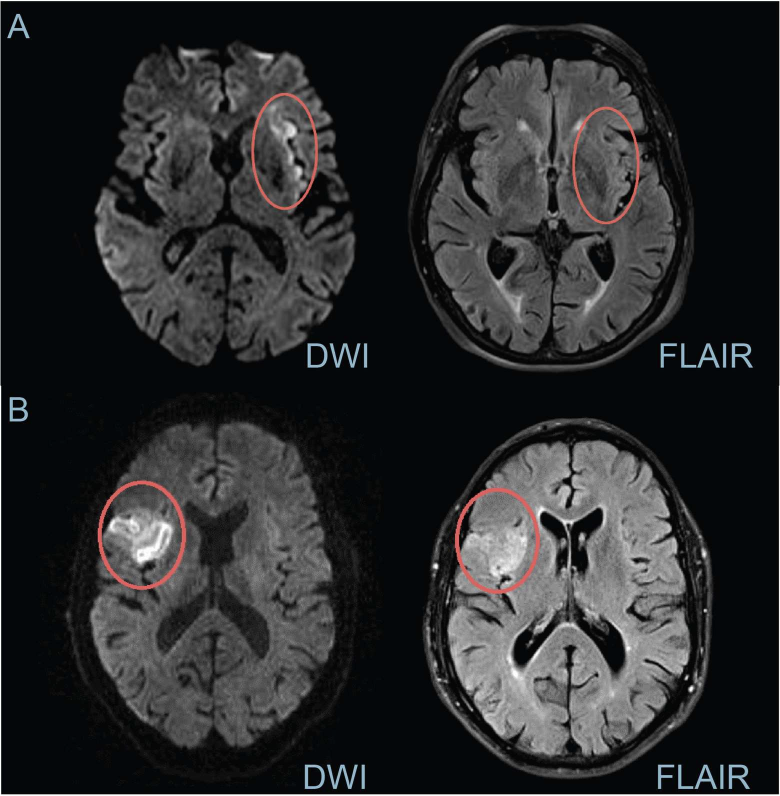
Fig. 4 Sample magnetic resonance (MR) images of an acute stroke using diffusion-weighted imaging (DWI) and fluid-attenuated inversion recovery (FLAIR) sequences. (A) Time from stroke onset is likely to be <4.5 h in patients with mismatched DWI and FLAIR scans (i.e. hyperintense lesion on DWI is consistent with reduced diffusivity due to cytotoxic oedema but FLAIR images show no signal abnormality).
- Time from stroke onset is likely to be >4.5 h in patients with visible lesions in both DWI and FLAIR MRI scans (i.e. hyperintense lesion on DWI is consistent with cytotoxic oedema induced by brain ischaemia and hyperintense signal on FLAIR, a sign of vasogenic oedema). DWI-FLAIR mismatch is commonly used in clinical trials to select patients for thrombolysis when the time of symptom onset is unknown. (Images courtesy of the Center for Stroke Research Berlin & the PRE-FLAIR )
Treatment
When left untreated, about two out of three stroke patients are either deceased or dependent after six months; modern treatment options lower this rate to about 40 %. For ischaemic stroke, reduction in stroke mortality and long-term disability seen over the past two decades among high-income countries is almost entirely due to five interventions which have been shown to be effective in at least one properly designed, randomised controlled trial:
- management of patients within a stroke unit (LANGHORNE et al. 1993), (ii) tissue plasminogen activator for intravenous thrombolysis within 4.5 hours of stroke onset (LEES et al. 2010), (iii) mechanical reopening of an occluded vessel with the help of vascular catheters, the so-called mechanical thrombectomy method, in particular for severely affected patients in whom a large brain vessel is blocked within 6 hours of stroke onset (BERKHEMER et al. 2015), (iv) aspirin within 48 hours of stroke onset (International Stroke Trial Collaborative Group 1997, JOHNSTON et al. 2018), and (v) decompressive surgery typically in younger patients with large middle cerebral artery (MCA) territory stroke (SCHWAB et al. 1998). Of these five treatments, the evidence is strongest for the long-term benefits of stroke unit treatment. Management within a stroke unit in the first days after stroke can be considered a complex organisational intervention. It comprises treatment by specialised multi-disciplinary staff, including specialised nursing and rehabilitation, as well as continuous monitoring of vital functions, fast access to imaging, and early initiation of secondary prevention (Fig. 5). Stroke unit treatment has been studied in ran- domised controlled trials since the 1990s and reduces death or dependency after one year by around 30 %.
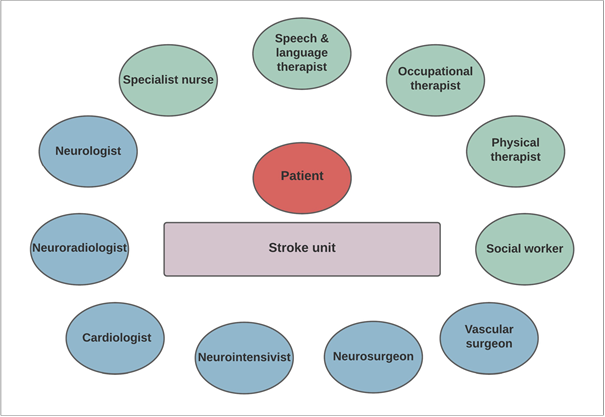
Fig. 5 Patient-centred model of specialised, interdisciplinary stroke unit care.
Tab. 2 Current treatment options of ischaemic stroke. The odds ratio represents the odds that death or dependency will occur given exposure to a particular treatment, compared to the odds of the outcome occurring in the absence of that exposure. The number needed to treat represents the average number of patients who need to be treated to prevent one additional bad outcome (e.g. the number of patients that need to be treated for one of them to benefit compared with a control in a clinical trial). n/a = not available
Percentage of acute stroke patients that can be targeted by this therapy
Odds ratio (death or dependency)
Number needed to treat
Reference
Stroke unit
70 % (-100 %)
0.75 (0.66 – 0.85)
15 (10 – 27)
(LANGHORNE et al. 2020)
Thrombolysis
15 % (-25 %)
0.76 (0.70 – 0.84)
16 (12 – 25)
(WARDLAW et al. 2009)
Mechanical thrombectomy
~10 % (-15 %)
0.62 (0.49 – 0.83)
8 (6 – 23)
(CHURCH et al. 2017)
Decompressive surgery (results for death only)
~0.5 %
0.18 (0.11 – 0.29)
2 (2 – 3)
(RAHME et al. 2012, GUL et al. 2018)
Aspirin
n/a
0.96
110
(International Stroke Trial Collaborative Group 1997)
Treatment of acute haemorrhagic stroke is geared towards limiting the mass effect of the bleeding and manage- ment of acute complications such as a decreased level of consciousness. Blood pressure is often elevated in patients suffering from a haemorrhagic stroke and should be acutely lowered to stop haematoma expansion. For patients taking anticoagulants or antiplatelet drugs, these should be urgently discontinued and anticoagulant effects should be reversed immediately with appropriate agents (HEMPHILL et al. 2018). After an initial emergency evaluation, patients should be managed in a dedicated stroke unit so that patient deterioration can be detected and reacted to swiftly, including invasive measures to reduce intracranial pressure by ventricular drainage or surgery. There remains a lack of clear criteria for the primary surgical management for removing a haemorrhage and decisions should be made on a per patient basis (HEMPHILL et al. 2018, Fig. 6).
Fig. 6 Flowchart depicting the acute stroke pathway
Local Solutions
In Germany, stroke mortality rates have decreased by 50 % since the 1990s (RÜCKER et al. 2018). This success was driven by local innovations and a coordinated national plan for fast access to specialised acute treatment and care within stroke units (LANGHORNE et al. 2020). In the past 30 years, more than 300 stroke units have been certified by the German Stroke Society and today, more than 70 % (BUSSE et al. 2013) of all stroke patients are treated in a certified stroke unit. Recently, interdisciplinary neurovascular specialist networks have been imple- mented nationally to improve care for complex and severe stroke cases. These neurovascular networks provide smaller hospitals, connected within the network, with fast access to expertise in the areas of neurology, neurosur- gery, and vascular surgery at a central coordinating centre. Hospitals in the network share common standards and referral pathways i.e. for mechanical thrombectomy or specialised neurointensive care and in many cases are directly linked through telemedicine (BUSSE et al. 2013).
Despite this success in making specialised care available, only ~15 % of acute stroke patients (WEBER et al. 2019) receive treatment with intravenous recombinant plasminogen activator (rTPA) and only 5 % receive mechanical thrombectomy with large variances between regions (WEBER et al. 2019). The benefits of thrombo- lysis and mechanical thrombectomy are time-dependent. Thrombolysis is limited to a narrow window of 4.5 hours after symptom onset (EMBERSON et al. 2014); mechanical thrombectomy is indicated for patients with large artery occlusion in the anterior circulation for up to 24 hours after symptom onset regardless of whether they received thrombolysis for the same event (NOGUEIRA et al. 2018).
Reasons for delays in initiating treatment include prehospital delays, such as the time it takes a patient to decide to call emergency services and the time from emergency call to arrival at the hospital, as well as in-hospital delays. To reduce in-hospital delays and increase the number of patients receiving thrombolysis, structured stroke alarm systems, including pre-notification of the arrival of emergency medical services (EMS), and single-call activation of dedicated stroke teams have been implemented successfully in many emergency care units, reducing door-to-treatment time to under 45 minutes (KÖHRMANN et al. 2011). Alongside similar initiatives in other regions of Germany, the Center for Stroke Research Berlin (CSB) was founded as an integrated centre for treatment and research to develop innovative concepts to improve acute and long-term care. Its research focuses on three goals: to protect the brain, prevent complications, and restore function. To further reduce the delay in initiating treatment, the CSB, together with the Berlin Fire Brigade, developed a specialised ambulance vehicle, the Stroke Emergency Mobile (STEMO), equipped with a CT scanner and point-of-care laboratory to allow for prehospital thrombolysis. This has shortened the time-to-treatment by 25 minutes and increased the number of patients treated with throm- bolysis by 50 % (KUNZ et al. 2016, Fig. 7). Moreover, STEMO treatment reduces long-term disability (EBINGER et al. 2021).
With the advent of mechanical thrombectomy at interventional centres and the availability of neurovascular networks, two approaches for patients with suspected large vessel occlusion have come up for debate: ‘drip and ship’, meaning primary transportation to the closest stroke unit and secondary transportation to an interventional centre if large vessel occlusion is confirmed, or the ‘direct to mothership’ approach with direct transportation of severely affected patients to a neurointerventional site (ABILLEIRA et al. 2019). In a simulation experiment using real-life data, researchers from the CSB demonstrated a favourable outcome for the ‘direct to mothership’ approach if the additional delay to thrombolysis is under 30 minutes in urban settings and under 50 minutes in rural settings (SCHLEMM et al. 2019, 2020). Correctly identifying these patients, however, remains a prerequisite for adequate care. To this end, the CSB has developed a telemedicine network for acute stroke care within the ANNOTeM project and has expanded it to include healthcare providers in rural areas across north-eastern Germany (WEBER et al. 2020). The Berlin Stroke Alliance was established by the CSB in 2008 to ensure close follow-up and optimal long-term care. It connects institutions along the continuum of care, providing a single point of contact for patients and improving patient education (Berliner Schlaganfall Allianz e.V. 2020).
Fig. 7 (A) Catchment areas of Stroke Emergency Mobile Units (STEMOs) stationed at three locations in Berlin. Insets show the STEMO vehicle (B) mounted with a mobile CT scanner (C). Adapted from (EBINGER et al. 2021). (Images courtesy of the Berlin Fire Brigade.)
An Emphasis on Stroke Prevention
Global stroke mortality and age-adjusted incidence declined during the last two decades mainly due to improve- ments in acute stroke care, effective prevention strategies, first-and-foremost treatment of hypertension, and anti- coagulation for atrial fibrillations. However, the overall stroke burden continues to increase rapidly in terms of absolute numbers of people affected by and living with stroke and stroke-related disabilities (FEIGIN et al. 2016a). This suggests that current primary prevention efforts for stroke are insufficient in stemming the tide of the growing stroke burden. Furthermore, stroke prevention strategies are mostly based on high-income country data available from registries and disease surveillance databases. It remains uncertain whether these strategies can be equally effective in low- and middle-income countries, where a younger age of onset, higher rates of haemorrhagic strokes, and increased exposure to modifiable risk factors, such as air pollution, indicate the need for population-specific stroke prevention strategies. Notably, the World Health Organization regards primary prevention as the most cost- effective strategy for reducing the overall stroke burden, especially in low-resource communities where access to emergency care and acute stroke treatment is limited.
Primary Prevention
Lifestyle changes, treatment with lipid-lowering drugs, antihypertensive medication or anticoagulation in patients with atrial fibrillation and additional risk factors are effective and cost-efficient for both primary and secondary prevention of stroke. The largest case-control study to date, which included 26,919 participants from 32 countries (INTERSTROKE Study) found a 47.9 % population-attributable risk of hypertension (99 % CI 45.1 – 50.6; 45.7 % (42.4 – 49.0) for ischaemic stroke and 56.4 % (52.0 – 60.6) for haemorrhagic stroke) (O’DONNELL et al. 2016). Antihypertensive therapy versus a placebo reduced the risk of stroke by 32 % (95 % CI 24 – 39). Atrial fibrillation contributes up to a 17.1 % population-attributable risk for ischaemic stroke (ibid.), but long-term treatment with anticoagulants can almost halve this risk in high-risk groups (FRIBERG et al. 2012). Interestingly, more than half of the modifiable risk factors can be mitigated by lifestyle changes, highlighting the importance of education and primary prevention.
Tab. 3 Leading modifiable risk factors for stroke, accounting for 91 % of population-attributable risk (O’DONNELL et al. 2016). Modified Alternative Healthy Eating Index, mAHEI.
Odds ratio (99 % confidence interval)
Population attributable risk (99 % confidence interval)
Hypertension
2.98 (2.72 - 3.28)
47.9 % (45.1 - 50.6)
Regular physical activity
0.60 (0.52 - 0.70)
35.8 % (27.7 - 44.7)
Apolipoprotein (Apo)B/ApoA1 ratio
1.84 (1.65 - 2.06) for highest vs lowest tercile
26.8 % (22.2 - 31.9) for top two terciles vs lowest tercile
Diet
0.60 (0.53 - 0.67) for highest vs lowest tercile of mAHEI
23.2 % (18.2 - 28.9) for lowest two terciles vs highest tercile of mAHEI
Waist-to-hip ratio
1.44 (1.27 - 1.64) for highest vs lowest tercile
18.6 % (13.3 - 25.3) for top two terciles vs lowest
Psychosocial factors
2.20 (1.78 - 2.72)
17.4 % (13.1 - 22·6)
Current smoking
1.67 (1.49 - 1.87)
12.4 % (10.2 - 14.9)
Cardiac causes (including atrial fibrillation)
3.17 (2.68 - 3.75)
9.1 % (8.0 - 10.2)
Alcohol consumption
2.09 (1.64 - 2.67) for high or heavy episodic intake vs non- or former drinker
5.8 % (3.4 - 9.7) for current drinker vs non- or former drinker
Diabetes mellitus
1.16 (1.05 - 1.30)
3.9 % (1.9 - 7.6)
Secondary Prevention
After an ischaemic stroke or TIA has occurred, it is paramount to aggressively target modifiable risk factors. In order to manage a non-cardioembolic acute stroke, antiplatelet therapy using aspirin, or a short-term dual antiplatelet therapy using a combination of aspirin and clopidogrel for patients with TIA or minor stroke, should be initiated as soon as possible after symptom onset. Aspirin monotherapy remains the mainstay of long-term secondary stroke prevention. Patients with atrial fibrillation should receive long-term anticoagulant therapy using an oral direct thrombin inhibitor or a factor Xa inhibitor following a careful risk-benefit assessment to avoid bleeding complications. Additionally, treatment with lipid-lowering drugs, such as statins can be effective even in patients without elevated cholesterol levels, reducing the risk of recurrent stroke by almost 20 % (TRAMACERE et al. 2019). For some causes of stroke, such as carotid artery stenosis, a narrowing of the main vessels supplying the brain, mostly caused by atherosclerosis, or a patent foramen ovale, i.e. a hole in the tissue that separates the left and the right upper chamber of the heart, there are specific interventions available for secondary prevention. However, overall adherence to chronic drug treatment regimens is low because access to safe and affordable medicine is limited in low- and middle-income countries that face the highest stroke burden. Meanwhile, mobile phones and mobile internet access have become ubiquitous in low- and middle-income countries, reaching people who, until now, have remained structurally excluded. Mobile technology is also increasingly being used in the healthcare sector to implement low-cost screening mechanisms for conditions that increase stroke risk and to target behavioural risk factors. Studies evaluating the impact and cost-effectiveness of mobile technology in reducing the burden of stroke are scarce (FEIGIN et al. 2016a), however there is rising evidence for successful prevention of non-communicable diseases in low- and middle-income countries using mobile technology.
Conclusion
More attention from national and global stakeholders, as well as from funding agencies, is needed to turn the tide of the growing stroke burden. They must support research and the implementation of effective primary and secondary prevention strategies as well as improve access to essential diagnostics and treatment. An emphasis on stroke prevention is urgently needed in low- and middle-income countries.
Author Contributions
JE, SK and ME conceptualised the article together. JE and SK wrote the first draft of the paper and ME made substantial reviews. All authors contributed to, reviewed, and approved the final draft.
References
ABILLEIRA, S., OSSA, N. P. DE LA, JIMENEZ, X., CARDONA, P., COCHO, D., PURROY, F., SERENA, J., SAN ROMÁN, L., URRA, X., VILARÓ, M., CORTÉS, J. GONZÁLEZ, J. A., CHAMORRO, Á., GALLOFRÉ, M., JOVIN, T., MOLINA, C., COBO, E., DÁVALOS, A., and RIBÓ, M.: Transfer to the local stroke center versus direct transfer to endovascular center of acute stroke patients with suspected large vessel occlusion in the catalan territory (RACECAT): Study protocol of a cluster randomized within a cohort trial. Int. J. Stroke 14/7, 734–744 (2019). doi:10.1177/1747493019852176 ANKARCRONA, M., DYPBUKT, J. M., BONFOCO, E., ZHIVOTOVSKY, B., ORRENIUS, S., LIPTON, S. A., and NICOTERA, P.: Glutamate-induced neuronal death: a succession of necrosis or apoptosis depending on mitochondrial function. Neuron. 15/4, 961–973 (1195). doi:10.1016/0896-6273(95)90186-8 ANRATHER, J., and IADECOLA, C.: Inflammation and stroke: an overview. Neurotherapeutics 13/4, 661–670 (2016). doi:10.1007/s13311-016- 0483-x ARONOWSKI, J., and ZHAO, X.: Molecular pathophysiology of cerebral hemorrhage. Stroke 42/6, 1781–1786 (2011). doi:10.1161/STROKEAHA.110.596718 ASCH, C. J. van, LUITSE, M. J., RINKEL, G. J., TWEEL, I. van der, ALGRA, A., and KLIJN, C. J.: Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. 9/2, 167–176 (2010). doi:10.1016/S1474-4422(09)70340-0 ASTRUP, J., SYMON, L., BRANSTON, N. M., and LASSEN, N. A.: Cortical evoked potential and extracellular K+ and H+ at critical levels of brain ischemia. Stroke 8/1, 51–57 (1977). doi:10.1161/01.str.8.1.51 BERKHEMER, O. A., FRANSEN, P., BEUMER, D., BERG, L. A., 60 further authors, DIPPEL, D. W. J., and MR Clean Investigators: A randomized trial of intraarterial treatment for acute ischemic stroke. N. Engl. J. Med. 372/1, 11–20 (2015). doi:10.1056/NEJMoa1411587 Berliner Schlaganfall Allianz e.V.: Homepage. Available at: https://www.schlaganfallallianz.de/ueber-die-bsa/fortbildung/ BOGOUSSLAVSKY, J., MELLE, G. V., and REGLI, F.: The Lausanne stroke registry: analysis of 1,000 consecutive patients with first stroke. Stroke. 19/9, 1083–1092 (2018). doi:10.1161/01.str.19.9.1083 BORNSTÄDT, D. VON, HOUBEN, T., SEIDEL, J. L., ZHENG, Y., DILEKOZ, E., QIN, T., SANDOW, N., KURA, S., EIKERMANN-HAERTER, K., ENDRES., M., BOAS, D. A., MOSKOWITZ, M. A., LO, E. H., DREIER, J. P., WOITZIK, J., SAKADŽIĆ, S., and AYATA, C.: Supply-demand mismatch transients in susceptible peri-infarct hot zones explain the origins of spreading injury depolarizations. Neuron. 85/5, 1117–1131 (2015). doi:10.1016/j.neuron.2015.02.007 BUSSE, O., RÖTHER, J., FAISS, J., HAMANN, G. F., HUPP, T., JANSEN, O., MEIXENBERGER, J., NEUMANN-HAEFELIN, T., SCHACKERT, G., and RINGELSTEIN, E. B.: Interdisziplinäres neurovaskuläres Netzwerk [Interdisciplinary neurovascular network: a new structure for treatment of stroke and other cerebrovascular diseases in Germany]. Nervenarzt 84/10, 1228–1232 (2013). doi:10.1007/s00115-013-3848-y CHAN, P. H.: Reactive oxygen radicals in signaling and damage in the ischemic brain. J. Cereb. Blood Flow Metab. 21/1, 2–14 (2001). doi:10.1097/00004647-200101000-00002 CHURCH, E. W., GUNDERSEN, A., GLANTZ, M. J., and SIMON, S. D.: Number needed to treat for stroke thrombectomy based on a systematic review and meta-analysis. Clin. Neurol. Neurosurg. 156, 83–88 (2017). doi:10.1016/j.clineuro.2017.03.005 CLARKE, D., and SKOLOFF, L.: Chapter 31: Circulation and Energy Metabolism of the Brain. In: SIEGEL, G. J., AGRANOFF, B. W., ALBERS, W., FISHER, S. K., and UHLER, M. D. (Eds.): Basic Neurochemistry. Molecular, Cellular and Medical Aspects. 6th Edition. Philadelphia: Lippincott-Raven 1999 Available at: https://www.ncbi.nlm.nih.gov/books/NBK20413/ CORDONNIER, C., DEMCHUK, A., ZIAI, W., and ANDERSON, C. S.: Intracerebral haemorrhage: current approaches to acute management. Lancet 392/10154, 1257–1268 (2018). doi:10.1016/S0140-6736(18)31878-6 CROSSLEY, N. A., SENA, E., GOEHLER, J., HORN, J., WORP, B. van der, BATH, P. M. W., MACLEOD, M., and DIRNAGL, U.: Empirical evidence of bias in the design of experimental stroke studies: a metaepidemiologic approach. Stroke 39/3, 929–934 (2008). doi:10.1161/STROKEAHA.107.498725 DANIEL, K., WOLFE, C. D. A., BUSCH, M. A., and MCKEVITT, C.: What are the social consequences of stroke for working-aged adults? Stroke 40/6, e431–e440 (2009). doi:10.1161/STROKEAHA.108.534487 DEGTEREV, A., HUANG, Z., BOYCE, M., LI, Y., JAGTAP, P., MIZUSHIMA, N., CUNY, G. D., MITCHISON, T. J., MOSKOWITZ, M. A., and YUAN, J.: Chemical inhibitor of nonapoptotic cell death with therapeutic potential for ischemic brain injury. Nat. Chem. Biol. 1/2, 112–119 (2005). doi:10.1038/nchembio711 DIRNAGL, U., IADECOLA, C., and MOSKOWITZ, M. A.: Pathobiology of ischaemic stroke: an integrated view. Trends Neurosci. 22/9, 391–397 (1999). doi:10.1016/s0166-2236(99)01401-0 DIRNAGL, U., and ENDRES, M.: Found in translation: preclinical stroke research predicts human pathophysiology, clinical phenotypes, and therapeutic outcomes. Stroke; a journal of cerebral circulation. 45/5, 1510–1518 (2014). doi:10.1161/STROKEAHA.113.004075 DREIER, J. P., and REIFFURTH, C.: The stroke-migraine depolarization continuum. Neuron. 86/4, 902–922 (2015). doi:10.1016/j.neuron.2015.04.004 EBINGER, M., SIEGERINK, B., KUNZ, A., WENDT, M., 27 further authors, ENDRES, M., AUDEBERT, H. J., and Berlin_PRehospital Or Usual Delivery in stroke care (B_PROUD) study group: Association between dispatch of mobile stroke units and functional outcomes among patients with acute ischemic stroke in Berlin. JAMA 325/5, 454–466 (2021). doi:10.1001/jama.2020.26345 EMBERSON, J., LEES, K. R., LYDEN, P., BLACKWELL, L., ALBERS, G., BLUHMKI, E., BROTT, T., COHEN, G., DAVIS, S., DONNAN, G., GROTTA, J., HOWARD, G., KASTE, M., KOGA, M., KUMMER, R. VON, LANSBERG, M., LINDLEY, R. I., MURRAY, G., OLIVOT, J. M., PARSONS, M., TILLEY, B., TONI, D., TOYODA, K., WAHLGREN, N., WARDLAW, J., WHITELEY, W., ZOPPO, G. J. del, BAIGENT, C., SANDERCOCK, P., HACKE, W., and Stroke Thrombolysis Trialists‘ Collaborative Group: Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet 384/9958, 1929–1935 (2014). doi:10.1016/S0140-6736(14)60584-5 ENDRES, M., ENGELHARDT, B., KOISTINAHO, J., LINDVALL, O., MEAIRS, S., MOHR, J. P., PLANAS, A., ROTHWELL, N., SCHWANINGER, M., SCHWAB, M. E., VIVIEN, D., WIELOCH, T., and DIRNAGL, U.: Improving outcome after stroke: overcoming the translational roadblock. Cerebrovasc. Dis. 25/3, 268 278 (2008). doi:10.1159/000118039 ENDRES, M., NAMURA, S., SHIMIZU-SASAMATA, M., WAEBER, C., ZHANG, L., GÓMEZ-ISLA, T., HYMAN, B. T., and MOSKOWITZ, M. A.: Attenuation of delayed neuronal death after mild focal ischemia in mice by inhibition of the caspase family. J. Cereb. Blood Flow Metab. 18/3, 238–247 (1998). doi:10.1097/00004647-199803000-00002 EYDING, J., BARTIG, D., WEBER, R., KATSANOS, A. H., WEIMAR, C., HACKE, W., and KROGIAS, C.: Inpatient TIA and stroke care in adult patients in Germany – retrospective analysis of nationwide administrative data sets of 2011 to 2017. Neurol. Res. Pract. 1, 39 (2019). doi:10.1186/s42466-019-0044-y FEIGIN, V. L., KRISHNAMURTHI, R. V., PARMAR, P., NORRVING, B., MENSAH, G. A., BENNETT, D. A., BARKER-COLLO, S., MORAN, A. E., SACCO, R. L., TRUELSEN, T., DAVIS, S., PANDIAN, J. D., NAGHAVI, M., FORUZANFAR, M. H., NGUYEN, G., JOHNSON, C. O., VOS, T., MERETOJA, A., MURRAY, C. J. L., ROTH, G. A., GBD 2013 Writing Group, and GBD 2013 Stroke Panel Experts Group: Update on the global burden of ischemic and hemorrhagic stroke in 1990-2013: The GBD 2013 Study. Neuroepidemiology 45/3, 161–176 (2015). doi:10.1159/000441085 FEIGIN, V. L., NORRVING, B., GEORGE, M. G., FOLTZ, J. L., ROTH, G. A., and MENSAH, G. A.: Prevention of stroke: a strategic global imperative. Nat. Rev. Neurol. 12/9, 501–512 (2016a). doi:10.1038/nrneurol.2016.107 FEIGIN, V. L., ROTH, G. A., NAGHAVI, M., PARMAR, P., KRISHNAMURTHI, R., CHUGH, S., MENSAH, G. A., NORRVING, B., SHIUE, I., NG, M., ESTEP, K., CERCY, K., MURRAY, C. J. L., FOROUZANFAR, M.H., and Global Burden of Diseases, Injuries and Risk Factors Study 2013 and Stroke Experts Writing Group: Global burden of stroke and risk factors in 188 countries, during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet Neurol. 15/9, 913–924 (2016b). doi:10.1016/S1474-4422(16)30073-4 FRIBERG, L., ROSENQVIST, M., and LIP, G. Y.H.: Net clinical benefit of warfarin in patients with atrial fibrillation. Circulation 125/19, 2298– 2307 (2012). doi:10.1161/CIRCULATIONAHA.111.055079 FROSCH. M. P., ANTHONY, D. C., and GIROLAMI, U. D.: The Central Nervous System. In: ROBBINS, S. L., KUMAR, V., ABBAS, A. K., COTRAN, S., and FAUSTO, N. (Eds.): Robbins and Cotran Pathologic Basis of Disease; pp 1313–1317. Philadelphia: Elsevier 2010. GUL, W., FULLER, H. R., WRIGHT, H., and SEN, J.: A systematic review and meta-analysis of the effectiveness of surgical decompression in treating patients with malignant middle cerebral artery infarction. World Neurosurg. 120, e902–e920 (2018). doi:10.1016/j.wneu.2018.08.189 HEMPHILL, J. C. 3rd, GREENBERG, S. M., ANDERSON, C. S., BECKER, K., BENDOK, B. R., CUSHMAN, M., FUNG, G. L., GOLDSTEIN, J. N., MACDONALD, R. L., MITCHELL, P. H., SCOTT, P. A., SELIM, M. H., WOO, D., American Heart Association Stroke Council, Council on Cardiovascular and Stroke Nursing, and Council on Clinical Cardiology: Guidelines for the management of spontaneous intracerebral hemorrhage. Stroke. 46/7, 2032–2060 (2018). doi:10.1161/STR.0000000000000069 HOUSE, A., KNAPP, P., BAMFORD, J., and VAIL, A.: Mortality at 12 and 24 months after stroke may be associated with depressive symptoms at 1 month. Stroke 32/3, 696–701 (2001). doi:10.1161/01.str.32.3.696 Institute for Health Metrics and Evaluation: GBD Results Tool, 2020. Available at: http://ghdx.healthdata.org/gbd-results-tool International Stroke Trial Collaborative Group: The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19 435 patients with acute ischaemic stroke. Lancet 349/9065, 1569–1581 (1997) JOHNSON, C. O., NGUYEN, M., ROTH, G. A., NICHOLS, E., 267 further authors, VOS, T., and MURRAY, C. J. L.: Global, regional, and national burden of stroke, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 18/5, 439–458 (2019). doi:10.1016/S1474-4422(19)30034-1 JOHNSTON, S. C., EASTON, J. D., FARRANT, M., BARSAN, W., CONWIT, R. A., ELM, J. J., KIM, A. S., LINDBLAD, A. S., PALESCH, Y. Y:, and Clinical Research Collaboration, Neurological Emergencies Treatment Trials Network, and the POINT Investigators: Clopidogrel and Aspirin in acute ischemic stroke and high-risk TIA. N. Engl. J. Med. 379/3, 215–225 (2018). doi:10.1056/NEJMoa1800410 KÖHRMANN, M., SCHELLINGER, P. D., BREUER, L., DOHRN, M., KURAMATSU, J. B., BLINZLER, C., SCHWAB, S., and HUTTNER, H. B.: Avoiding in hospital delays and eliminating the three‐hour effect in thrombolysis for stroke. Int. J. Stroke 6/6, 493–497 (2011). doi:10.1111/j.1747-4949.2011.00585.x KUNZ, A., EBINGER, M., GEISLER, F., ROZANSKI, M., WALDSCHMIDT, C., WEBER, J. E., WENDT, M., WINTER, B., ZIESCHANG, K., FIEBACH, B., VILLRINGER, K., ERDUR, H., SCHEITZ, J. F., TÜTÜNCÜ, S., BOLLWEG, K., GRITTNER, U., KACZMAREK, S., ENDRES, M., NOLTE, C. H., and AUDEBERT, H. J.: Functional outcomes of pre-hospital thrombolysis in a mobile stroke treatment unit compared with conventional care: an observational registry study. Lancet Neurol. 15/10, 1035–1043 (2016). doi:10.1016/S1474-4422(16)30129-6 LANGHORNE, P., RAMACHANDRA, S., and Stroke Unit Trialists’ Collaboration: Organised inpatient (stroke unit) care for stroke: network meta‐analysis. Cochrane Database Syst. Rev. 4/4, CD000197 (2020). doi:10.1002/14651858.CD000197.pub4. LANGHORNE, P., WILLIAMS, B. O., GILCHRIST, W., and HOWIE, K.: Do stroke units save lives? Lancet 342/8868, 395–398 (1993). doi:10.1016/0140-6736(93)92813-9 LEES, K. R., BLUHMKI, E., KUMMER, R. VON, BROTT, T. G., TONI, D., GROTTA, J. C., ALBERS, G. W., KASTE, M., MARLER, J. R., HAMILTON, A., TILLEY, B. C., DAVIS, S. M., DONNAN, G. A. HACKE, W., ECASS, ATLANTIS, NINDS and EPITHET rt-PA Study Group, ALLEN, K., MAU, J., MEIER, D., ZOPPO, G. del, SILVA, D. A. De, BUTCHER, K. S., PARSONS, M. W., BARBER, P. A., LEVI, C., BLADIN, C., and BYRNES, G.: Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet 375/9727, 1695–1703 (2010). doi:10.1016/S0140-6736(10)60491-6 LUENGO-FERNANDEZ, R., PAUL, N. L. M., GRAY, A. M., PENDLEBURY, S. T., BULL, L. M., WELCH, S. J. V., CUTHBERTSON, F. C., ROTHWELL, P. M., and Oxford Vacular Study: Population-based study of disability and institutionalization after transient ischemic attack and stroke. Stroke 44/10, 2854–2861 (2013). doi:10.1161/STROKEAHA.113.001584 LUENGO-FERNANDEZ, R., VIOLATO, M., CANDIO, P., and LEAL, J.: Economic burden of stroke across Europe: A population-based cost analysis. Eur. Stroke J. 5/1, 17–25 (2019). doi:10.1177/2396987319883160 MACLEOD, M. R., WORP, H. B. van der, SENA, E. S., HOWELLS, D. W., DIRNAGL, U., and DONNAN, G. A.: Evidence for the efficacy of NXY- 059 in experimental focal cerebral ischaemia is confounded by study quality. Stroke 39/10, 2824–2829 (2008). doi:10.1161/STROKEAHA.108.515957 MIES, G., IIJIMA, T., and HOSSMANN, K. A.: Correlation between peri-infarct DC shifts and ischaemic neuronal damage in rat. Neuroreport 4/6, 709–711 (1993). doi:10.1097/00001756-199306000-00027 NEHER, J. J., NENISKYTE, U., ZHAO, J.-W., BAL-PRICE, A., TOLKOVSKY, A. M., and BROWN, G. C.: Inhibition of icroglial phagocytosis is sufficient to prevent inflammatory neuronal death. J. Immunol. 186/8, 4973–4983 (2011). doi:10.4049/jimmunol.1003600 NOGUEIRA, R. G., JADHAV, A. P., HAUSSEN, D. C., BONAFE, A., 41 further authors, SAVER, J. L., JOVIN, T. G., for the DAWN Trial Investigators: Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N. Engl. J. Med. 378/1, 11–21 (2018). doi:10.1056/NEJMoa1706442 O’COLLINS, V. E., MACLEOD, M. R, DONNAN, G. A., HORKY, L. L., WORP, B. H. van der, and HOWELLS, D. W.: 1,026 experimental treatments in acute stroke. Ann. Neurol. 59/3, 467–477 (2006). doi:10.1002/ana.20741 O’DONNELL, M. J., CHIN, S. L., RANGARAJAN, S., XAVIER, D., 40 further authors, PARE, G., YUSUF, S., and INTERSTROKE investigators: Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case- control study. Lancet 388/10046, 761–775 (2016). doi:10.1016/S0140-6736(16)30506-2 RAHME, R., CURRY, R., KLEINDORFER, D., KHOURY, J. C., RINGER, A. J., KISSELA, B. M., ALWELL, K., MOOMAW, C. J., FLAHERTY, M. L., KHATRI, P., WOO, D., FERIOLI, S., BRODERICK, J., and ADEOYE, O.: How often are patients with ischemic stroke eligible for decompressive hemicraniectomy? Stroke 43/2, 550–552 (2012). doi:10.1161/STROKEAHA.111.635185 RAMOS-CABRER, P., CAMPOS, F., SOBRINO, T., and CASTILLO, J.: Targeting the ischemic penumbra. Stroke 42/1 Suppl., 7–11 (2011). doi:10.1161/STROKEAHA.110.596684 ROGER, V. L., GO, A. S., LLOYD-JONES, D. M., ADAMS, R. J., 35 further authors, WONG, N. D., WYLIE-ROSETT, and American Heart Association Statistics Committee and Stroke Statistics Subcommittee: Heart disease and stroke statistics–2011 update: a report from the American Heart Association. Circulation 123/4, e18–e209 (2011). doi:10.1161/CIR.0b013e3182009701 ROGER, V. L., GO, A. S., LLOYD-JONES, D. M., BENJAMIN, E. J., 31 further authors, WOO, D., TURNER, M. B., and American Heart Association Statistics Committee and Stroke Statistics Subcommittee: Executive summary: Heart disease and stroke statistics–2012 Update: a report from the American Heart Association. Circulation 125/1, 188–197 (2012). doi:10.1161/CIR.0b013e3182456d46 RÜCKER, V., WIEDMANN, S., O’FLAHERTY, M., BUSCH, M. A., and HEUSCHMANN, P. U.: Decline in regional trends in mortality of stroke subtypes in Germany from 1998 to 2015. Stroke 49/11, 2577–2583 (2018). doi:10.1161/STROKEAHA.118.023193 SALAYCIK, K. J., KELLY-HAYES, M., BEISER, A., NGUYEN, A.-H., BRADY, S. M., KASE, C. S., and WOLF, P. A.: Depressive symptoms and risk of stroke: the Farmington Study. Stroke 38/1, 16–21 (2007). doi:10.1161/01.STR.0000251695.39877.ca SCHLEMM, L., ENDRES, M., and NOLTE, C. H.: Bypassing the closest stroke center for thrombectomy candidates: What additional delay to thrombolysis is acceptable? Stroke 51/3, 867–875 (2020). doi:10.1161/STROKEAHA.119.027512 SCHLEMM, L., SCHLEMM, E., NOLTE, C. H., and ENDRES, M.: Pre-hospital triage of acute ischemic stroke patients–importance of considering more than two transport options. Front Neurol. 10/437, eCollection 2019. doi:10.3389/fneur.2019.00437 SCHWAB, S., STEINER, T., ASCHOFF, A., SCHWARZ, S., STEINER, H. H., JANSEN, O., and HACKE, W.: Early hemicraniectomy in patients with complete middle cerebral artery infarction. Stroke 29/9, 1888–1893 (1998). doi:10.1161/01.str.29.9.1888 SENNFÄLT, S., NORRVING, B., PETERSSON, J., and ULLBERG, T.: Long-term survival and function after stroke. Stroke 50/1, 53–61 (2019). doi:10.1161/STROKEAHA.118.022913 SINGHAL, A. B., BILLER, J., ELKIND, M. S., FULLERTON, H. J., JAUCH, E. C., KITTNER, S. J., LEVINE, D. A., and LEVINE, S. R.: Recognition and management of stroke in young adults and adolescents. Neurology 81/12, 1089–1097 (2013). doi:10.1212/WNL.0b013e3182a4a451 SUN, M.-S., JIN, H., SUN, X., HUANG, S., ZHANG, F.-L., GUO, Z.-N., and YANG, Y.: Free radical damage in ischemia-reperfusion injury: an obstacle in acute ischemic stroke after revascularization therapy. Oxid. Med. Cell Longev. 2018/3804979, 1–17 (2018). doi:10.1155/2018/3804979 The GBD 2016 Lifetime Risk of Stroke Collaborators, FEIGIN, V. L., NGUYEN, G., CERCY, K., JOHNSON, C. O., 209 further authors, MURRAY, J. L., and ROTH, G. A.: Global, regional, and country-specific lifetime risks of stroke, 1990 and 2016. N. Engl. J. Med. 379/25, 2429– 2437 (2018). doi:10.1056/NEJMoa1804492 THOMALLA, G., SIMONSEN, C. Z., BOUTITIE, F., ANDERSEN, G., BERTHEZENE, Y., CHENG, B., CHERIPELLI, B., CHO, T.-H., FAZEKAS, F., FIEHLER, J., FORD, I., GALINOVIC, I., GELLISSEN, S., GOLSARI, A., GREGORI, J., GÜNTHER, M., GUIBERNAU, J., HÄUSLER, K. G., HENNERICI, M., KEMMLING, A., MARSTRAND, J., MODRAU, B., NEEB, L., OSSA, N. P. DE LA, PUIG, J., RINGLEB, P., ROY, P., SCHEEL, E., SCHONEWILLE, W., SERENA, J., SUNAERT, S., VILLRINGER, K., WOUTERS, A., THIJS, V., EBINGER, M., ENDRES, M., FIEBACH, J. B., LEMMENS, R., MUIR, K. W., NIGHOGHOSSIAN, N., PEDRAZA, S., and GERLOFF, C. for the WAKE-UP Investigators: MRI-guided thrombolysis for stroke with unknown time of onset. N. Engl. J. Med. 379/7, 611–622 (2018). doi:10.1056/NEJMoa1804355 TRAMACERE, I., BONCORAGLIO, G. B., BANZI, R., GIOVANE, C. D., KWAG, K. H., SQUIZZATO, A., and MOJA, L.: Comparison of statins for secondary prevention in patients with ischemic stroke or transient ischemic attack: a systematic review and network meta-analysis. BMC Med. 17/1, 67 (2019). doi:10.1186/s12916-019-1298-5 WANG, P., SHAO, B.-Z., DENG, Z., CHEN, S., YUE, Z., and MIAO, C.-Y.: Autophagy in ischemic stroke. Prog. Neurobiol. 163–164, 98–117 (2018). doi:10.1016/j.pneurobio.2018.01.001 WARDLAW, J. M., MURRAY, V., BERGE, E., and ZOPPO, G. J. DEL: Thrombolysis for acute ischaemic stroke. Cochrane Database Syst. Rev. 2014/7, CD000213 (2014). doi:10.1002/14651858.CD000213.pub3 WEBER, J. E., ANGERMAIER, A., BOLLWEG, K., ERDUR, H., ERNST, S., FLÖEL, A., GORSKI, C., KANDIL, F. I., KINZE, S., KLEINSTEUBER, K., KUETH, T., SCHMEHL, I., THEEN, S., ENDRES, M., and AUDEBERT, H. J., for the ANNOTeM-consortium: Acute neurological care in north- east Germany with telemedicine support (ANNOTeM): protocol of a multi-center, controlled, open-label, two-arm intervention study. BMC Health Serv. Res. 20/1, 755 (2020). doi:10.1186/s12913-020-05576-w WEBER, R., EYDING, J., KITZROW, M., BARTIG, D., WEIMAR, C., HACKE, W., and KROGIAS, C.: Distribution and evolution of acute inter- ventional ischemic stroke treatment in Germany from 2010 to 2016. Neurol. Res. Pract. 1/4, eCollection 2019. doi:10.1186/s42466-019- 0010-8 WOITZIK, J., HECHT, N., PINCZOLITS, A., SANDOW, N., MAJOR, S., WINKLER, M. K. L., WEBER-CARSTENS, S., DOHMEN, C., GRAF, R., STRONG A. J., DREIER, J. P., and VAJKOCZY, P., for the COSBID study group: Propagation of cortical spreading depolarization in the human cortex after malignant stroke. Neurology 80/12, 1095–1102 (2013). doi:10.1212/WNL.0b013e3182886932 World Health Organization: Leading causes of death and disability. A visual summary of global and regional trends 2000–2019. Available at: https://www.who.int/data/stories/leading-causes-of-death-and-disability-2000-2019-a-visual-summary